Recto-Vaginal Fistula
Recto-Vaginal Fistula
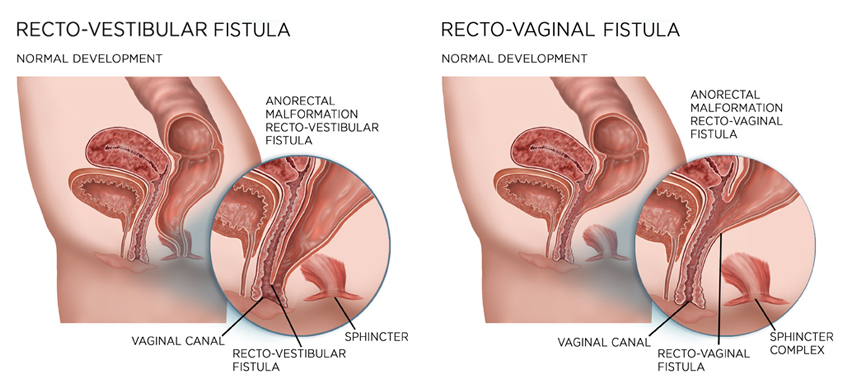
A recto-vaginal fistula - as the name indicates is a fistula, an abnormal connection between the rectum & vagina. The opening between the rectum & the vagina will allow the passage of faeces or flatus (gas) from the rectum to the vagina, creating an unhygienic, embarrassing and stressful condition for the patient. Not only there may be flatus and faecal matter being discharged / leaking out of the vagina, but it may lead to recurrent urinary and vaginal infections.
Recto-vaginal fistula can develop in women, young girls who are victims of forced sex. However, the most common cause found in women specially of developing and underdeveloped countries (in conditions where there is inadequate health care), is trauma during child birth r infection or tear of an episiotomy. This type of recto-vaginal fistulas is termed as "Obstetric fistula". The cause may be tears in the perineum that extend to the bowel, following a long & difficult labour. Obstetric fistula may involve injury to the anal sphincter also – this making matters more serious.
Causes
- Recto-vaginal fistulas are sometimes secondary manifestations / complication of certain other disease.
- They may be extension of carcinoma of rectum, cervix or vagina
- Having Crohn's disease increases the risk of a women to develop a recto-vaginal fistula
- In rare cases it may develop due to an underlying diverticular diseases or lymphogranuloma venereum
- As complication of ano-rectal abscess, Ulcerative colitis etc
Cancer or radiation treatment in pelvic area. A tumour in the uterus, cervix, vagina, rectum or anal canal may the cause of recto-vaginal fistula. Even its treatment – the radiation therapy (in the pelvic area) increases the risk of developing a recto-vaginal fistula. A recto-vaginal fistula caused due to radiation usually manifests within two years of the treatment. The patient may experience pain in the rectum, anus, pelvic region bloody diarrhoea or blood in the stool prior to the development of the fistula.
In rare cases infections in anus, rectum or vagina may lead to recto-vaginal fistula
Symptoms
Symptoms & their intensity may vary a little depending upon the type / size and location of the fistula. Low recto-vaginal fistula s may show mild symptoms where as high recto-vaginal fistula may create significant problems regarding hygiene, incontinence and other infections.
Symptoms may include:
- Irritation or pain in the vulva, vagina and the area between the vulva & vagina (perineum)
- Foul smelling , vaginal discharge may be yellowish or brownish or blood stained
- Passage of gas, stool or pus from the vagina
- Pain during sexual activity
- Recurrent vaginal and/or urinary track infection
Types
Usually the recto-vaginal fistulas are classified based on their length and the position of the opening inside the rectum.
They are classified as:
- Low recto-vaginal fistulas
- High recto-vaginal fistulas
- Intermediate recto-vaginal fistulas
- Probing
- A fine – malleable probe (a thick wire like instrument) may be passed through the opening to access the fistulous track.
Further investigations required:
Sometimes the opening of the fistula may be found during the physical examination or examination – probing may be too painful to complete the examination. In such cases and to confirm the diagnosis and plan for the surgery some other tests may be necessary to evaluate the recto-vaginal fistula.
Water & air test
Blue dye test- A blue dye is injected into the rectum and the tampon placed in the vagina , staining on the tampon indicates a presence of a fistula
Contrast test – Vaginogram, Barium enema, Ultra sound – ano-rectal ultra sound can help evaluate the involvement of sphincters
Computerised tomography (CT) – A CT scan of the pelvis can help locate the fistula & also its causes.
Magnetic resonance imaging (MRI) can help locate the fistula & can also how involvement of other pelvic organs, presence of tumour etc.
Ano-rectal manometry- helps planning the surgery.
Other tests like Colonoscopy, biopsy of the involved tissues helps to confirm underlying disease.
Treatment options
- Conventional
- Medical therapy
- Local hygiene care
- Draining of the abscess
- Antibiotics
- High fibre diet
(Specially obstetric fistula) some recto-vaginal fistulas may heal with medical treatment, but many may persist. If the fistula persists for over 11 to 12 weeks, surgery is considered
Surgical – Operative procedure will vary depending upon the causative factors
Complications
- Physical complications include
- Daily problems with hygiene
- Irritation, inflammation of vagina, vulva, perineum & skin of Perineal region
- Infection / abscess at the site
- Incontinence
In cases where the patient has Crohn's diseases, there is a possibility of the patient developing another fistula